US Measles Outbreak Surpasses 1,700 Cases as Utah Becomes New Epicenter
The US measles outbreak has crossed 1,714 cases in 2026, with Utah now driving national transmission as South Carolina's outbreak winds down.

Overview
The United States is experiencing its most significant measles resurgence in years. As of early April 2026, the national case count has climbed to 1,714 confirmed infections, according to reporting by the Center for Infectious Disease Research and Policy (CIDRAP). The outbreak, which has spread across multiple states, reflects deepening gaps in population immunity in certain communities — a pattern that public health officials have warned about for years as routine childhood vaccination rates have plateaued or declined in pockets of the country.
Measles, caused by the Rubeola virus, is one of the most contagious pathogens known to medicine. A single infectious individual can transmit the virus to up to 18 susceptible contacts in an unvaccinated population. That extraordinary transmission potential means even modest drops in vaccination coverage — below the roughly 95% threshold needed for herd immunity — can allow the virus to find and exploit vulnerable clusters. What is unfolding across the United States in 2026 is a textbook demonstration of that dynamic.
Current Situation
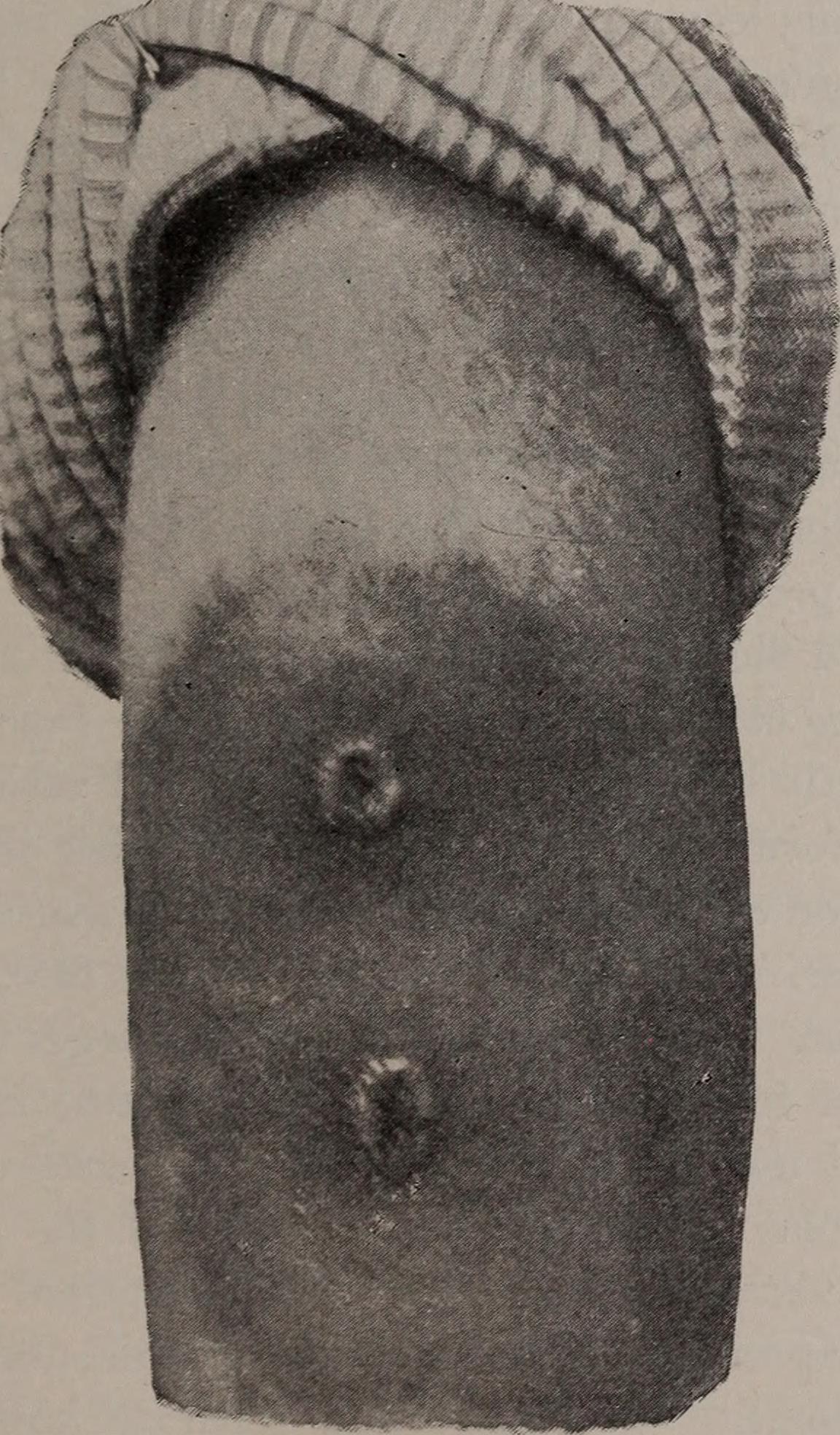 Image: Wikimedia Commons
Image: Wikimedia Commons
The pace of transmission, while showing some regional variation, has remained consistent at the national level. CIDRAP reported 43 new cases in the week ending April 10, bringing the cumulative 2026 total to 1,714 infections. That weekly figure, while not a dramatic spike, reflects the ongoing difficulty authorities face in interrupting chains of transmission.
The most striking data point in recent weeks involves Utah. In the three-week period ending approximately April 3, the state recorded 142 new infections — a number that exceeds Utah’s entire measles case count for all of 2025 (197 cases) in less than a month, according to CIDRAP. In the seven-day stretch leading up to April 3 alone, 73 of the nation’s 96 new cases were reported in Utah, illustrating how concentrated and rapid local transmission can become once the virus establishes itself in an under-immunized community.
Death toll data and case fatality rates for the current outbreak have not been specified in available CIDRAP reports, though measles carries well-documented risks of serious complications — including pneumonia, encephalitis, and death — particularly in unvaccinated children under five, immunocompromised individuals, and pregnant women.
Affected Regions
The geographic picture of this outbreak has shifted meaningfully over the past several weeks. South Carolina, which had been one of the more active outbreak states earlier in the year, has gone two full weeks without a newly reported case as of early April, according to CIDRAP — a sign that the intervention and containment efforts there are taking hold. Epidemiologically, a two-week window without new cases is significant for measles, given its incubation period of roughly 10 to 14 days; it suggests that active chains of transmission may have been broken.
Utah has absorbed much of that national transmission burden, becoming what CIDRAP now characterizes as the epicenter of the US outbreak. The state recorded 24 new cases in just five days in the period ending April 8. The concentration of cases in a single state at this velocity raises legitimate concern about community-level immunization gaps — whether due to philosophical vaccine exemptions, access barriers, or delayed catch-up vaccination schedules.
Beyond the active outbreak states, Chicago has also entered the picture. Health officials issued an alert following a potential measles exposure at a major airport, according to CIDRAP’s April 1 report. Airport exposures are of particular concern to epidemiologists because they can seed geographically dispersed transmission chains: a single infectious traveler passing through a crowded terminal can expose dozens of people who then disperse across the country or internationally before symptoms appear. Whether the Chicago airport exposure generated secondary cases was not confirmed in available reporting.
Risk Assessment
 Image: Wikimedia Commons
Image: Wikimedia Commons
Measles transmits through respiratory droplets and aerosolized particles that can remain infectious in the air for up to two hours after an infected person has left a space. This airborne persistence makes the virus exceptionally difficult to contain in dense settings like schools, religious gatherings, healthcare facilities, and transit hubs.
The populations most at risk in the current outbreak include:
- Unvaccinated children, particularly in communities where exemption rates are elevated
- Infants under 12 months, who are too young to have received the standard MMR vaccination
- Immunocompromised individuals, for whom vaccination may not produce adequate protection
- Pregnant women, who face elevated risk of complications if infected
- Adults with uncertain vaccination histories, a cohort often overlooked in outbreak response messaging
The two-dose MMR (measles-mumps-rubella) vaccine is approximately 97% effective against measles when both doses are received. The challenge is not the vaccine’s efficacy but the distribution of immunity across populations. Pockets of under-vaccination — whether clustered geographically, socially, or by age cohort — provide the virus with the opening it needs.
The airport exposure in Chicago is also a reminder that measles does not respect geographic containment lines. As long as there is active community transmission in the United States, the risk of seeding new outbreaks in previously unaffected cities remains real.
Prevention & Response
Public health guidance has emphasized a consistent set of precautionary steps as the outbreak continues to evolve. CIDRAP, drawing on expert commentary, has urged members of the public to familiarize themselves with the distinction between measles and influenza symptoms — a clinically important point, since the early prodromal stage of measles (featuring fever, cough, runny nose, and conjunctivitis) can be easily mistaken for flu.
The key clinical differentiator is the characteristic measles rash: a red, blotchy eruption that typically begins at the hairline and spreads downward over the body, appearing roughly three to five days after the onset of fever. Koplik spots — small white lesions on the inner cheek — are pathognomonic for measles and may appear before the rash. Experts advise that anyone suspecting measles exposure or symptoms should call ahead before visiting a clinic or emergency room to prevent inadvertent exposure of other patients in waiting areas.
State health departments in Utah and elsewhere have been conducting case investigations, contact tracing, and targeted vaccination outreach. In areas with active transmission, health officials typically recommend post-exposure prophylaxis — either MMR vaccine (within 72 hours of exposure) or immune globulin (within six days) — for susceptible contacts.
At the federal level, the Centers for Disease Control and Prevention (CDC) maintains surveillance and provides technical support to state health departments managing outbreak response. The national vaccination schedule recommends the first MMR dose at 12 to 15 months and the second at 4 to 6 years. Catch-up vaccination is available for older children and adults who missed either dose.
For travelers, the CDC advises ensuring full vaccination before international travel, but the current data underscore that domestic travel within the United States also carries exposure risk while community transmission remains active.
The overarching public health message at this stage is straightforward: verify your vaccination status. Two doses of MMR vaccine remain the most reliable protection available, and the current outbreak trajectory suggests that the virus will continue to find unprotected individuals until vaccination coverage is meaningfully reinforced in the communities driving transmission.
Sources
- CIDRAP — US measles total surpasses 1,700 cases (April 10, 2026)
- CIDRAP — US nears 1,700 measles cases, with 73 new infections in Utah (April 3, 2026)
- CIDRAP — South Carolina sees no new measles activity as Utah becomes epicenter of US outbreaks (April 8, 2026)
- CIDRAP — End in sight for South Carolina’s measles outbreak; Chicago on alert after potential airport exposure (April 1, 2026)
- CIDRAP — Are your symptoms caused by the flu or measles? What to do before going to the doctor (April 10, 2026)
Sources
- CIDRAP — US measles total surpasses 1,700 cases ↗
- CIDRAP — US nears 1,700 measles cases, with 73 new infections in Utah ↗
- CIDRAP — South Carolina sees no new measles activity as Utah becomes epicenter ↗
- CIDRAP — End in sight for South Carolina's measles outbreak; Chicago on alert ↗
- CIDRAP — Are your symptoms caused by the flu or measles? ↗