CDC Testing Pause Strains Mpox Surveillance as Global Cases Continue
CDC halts mpox and rabies testing amid efficacy review, shifting burden to state labs as global transmission persists into 2026.

Overview
Mpox — formerly known as monkeypox — remains an active global public health concern heading into the second quarter of 2026, with transmission reported across multiple continents. Against this backdrop, the Centers for Disease Control and Prevention (CDC) has introduced a significant operational disruption: a pause on its own diagnostic testing for mpox and a range of other pathogens, including rabies. The decision, attributed to an ongoing internal review of testing efficacy, is redirecting an unfamiliar burden onto state-level public health laboratories at a moment when robust surveillance capacity is arguably most needed.
The confluence of continued global spread and a contraction in federal diagnostic infrastructure raises legitimate questions about the United States’ ability to detect, characterize, and respond to mpox cases in a timely fashion. Public health officials and infectious disease specialists are watching the situation carefully, though state laboratories have so far moved to absorb the shortfall.
Current Situation
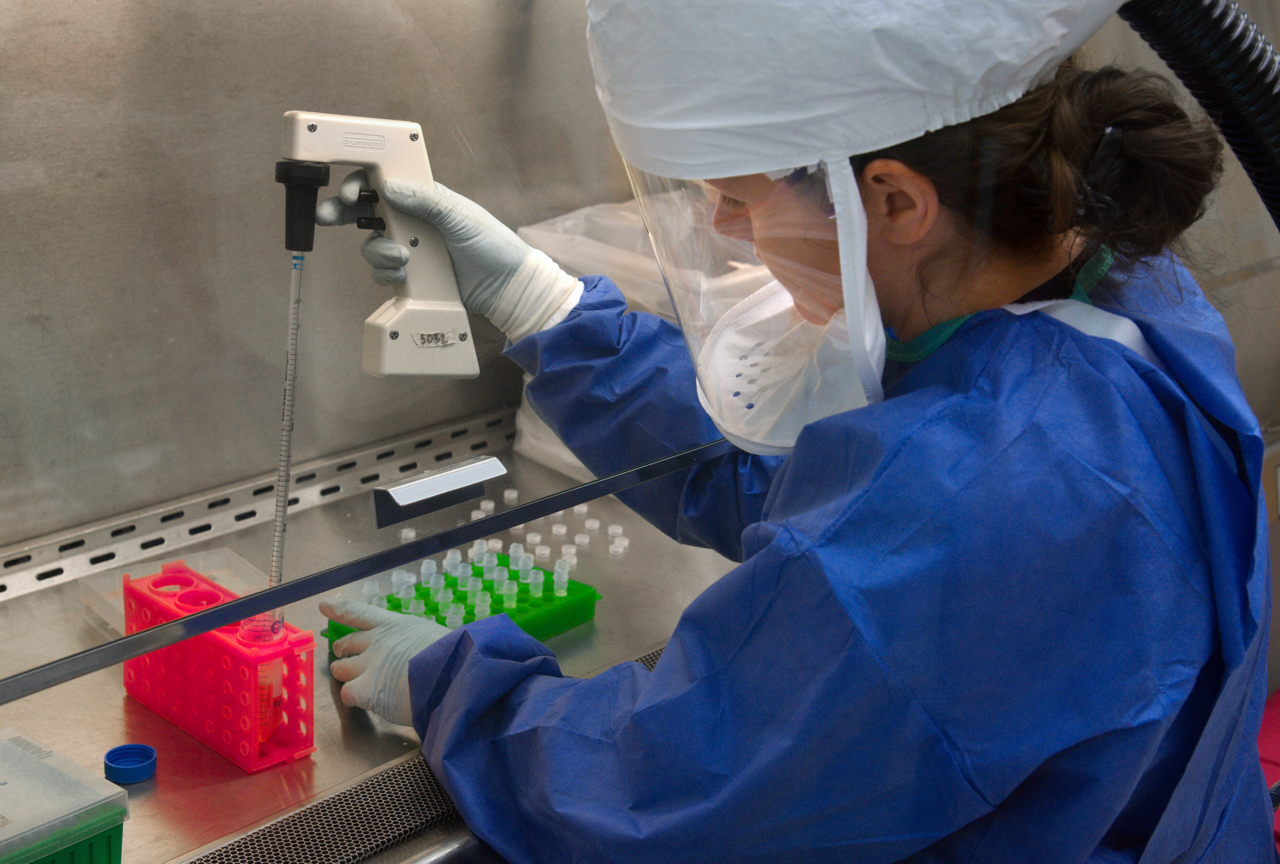 Image: Wikimedia Commons
Image: Wikimedia Commons
According to the European Centre for Disease Prevention and Control (ECDC), which publishes a detailed epidemiological overview of worldwide mpox transmission on a monthly basis as part of its weekly threat reports, global transmission of the virus has continued without interruption into 2026. The ECDC’s reporting framework tracks both Clade I and Clade II strains, monitoring case counts, geographic spread, and evolving outbreak dynamics across affected regions.
The ECDC does not publish a single cumulative global figure in its overview summaries; rather, it situates mpox within a broader threat assessment that is updated continuously. What the data consistently shows, however, is that mpox is not a resolved outbreak — it is an ongoing, multi-focal transmission event requiring sustained surveillance infrastructure.
On the domestic front, the situation changed materially in early April 2026 when the CDC announced it was pausing diagnostic testing for mpox alongside several other pathogens. CIDRAP (the Center for Infectious Disease Research and Policy at the University of Minnesota) reported the development on April 3, noting that the CDC’s pause is tied to a broad review of its testing efficacy — an administrative process that nonetheless carries real-world consequences for disease detection. The scale and anticipated duration of the pause have not been publicly specified in detail.
Affected Regions
Mpox transmission in 2026 reflects the bifurcated epidemiology that has characterized the disease since the 2022 global outbreak reshaped understanding of its spread. Clade I mpox, historically associated with Central Africa and carrying a higher case fatality rate, continues to circulate in endemic zones in the Democratic Republic of Congo and neighboring countries. The DRC has been the epicenter of the most severe ongoing transmission, and spillover into bordering nations has been documented in prior ECDC reporting cycles.
Clade II mpox, the strain responsible for the 2022 multicountry outbreak, has shown more diffuse global presence, with cases reported across Europe, the Americas, and parts of Asia. While the acute emergency of 2022 has subsided, Clade II has not been eliminated, and sporadic clusters continue to emerge in countries with incomplete vaccination coverage or among populations who did not receive immunization during the original response effort.
Within the United States, the CDC testing pause introduces geographic uncertainty. State public health laboratories — many of which expanded their mpox testing capacity during and after the 2022 outbreak — are now the primary diagnostic infrastructure for federal-level surveillance. Their capacity varies considerably by state, and the transition from a centralized federal reference laboratory to a distributed state-level system inevitably introduces variability in turnaround times, sensitivity, and reporting consistency.
Risk Assessment
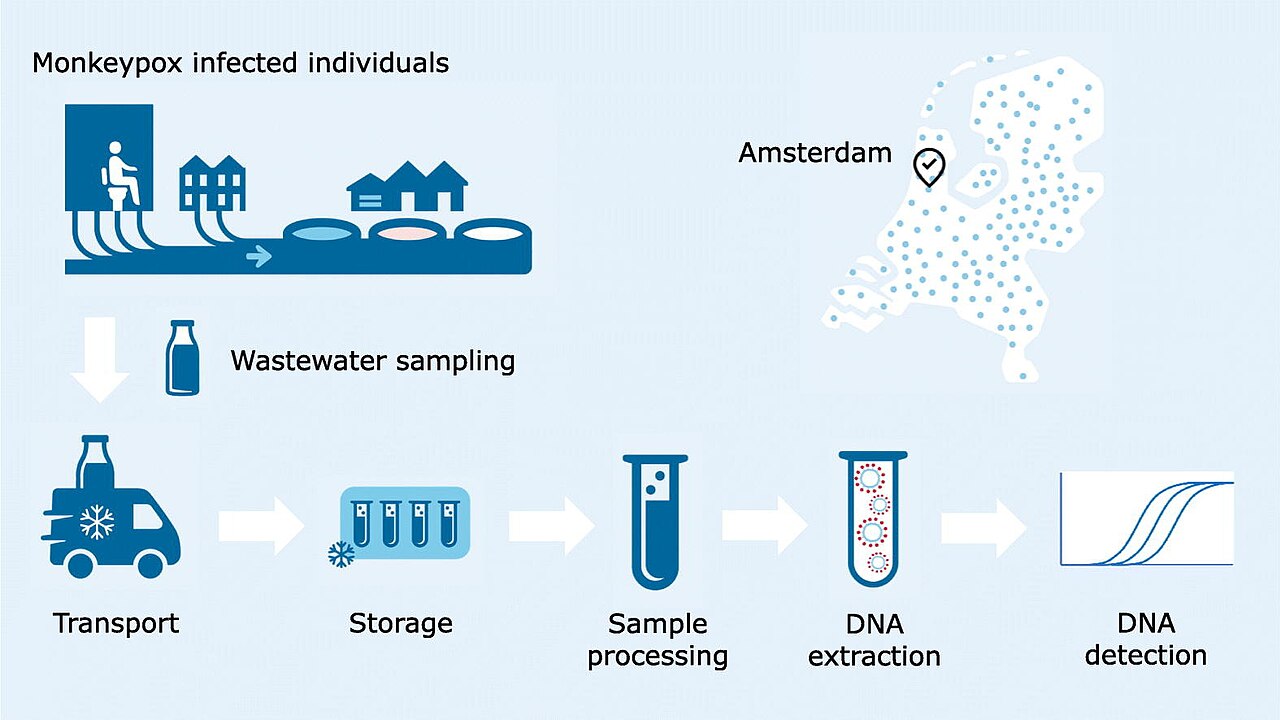 Image: Wikimedia Commons
Image: Wikimedia Commons
The World Health Organization (WHO) has maintained an elevated global risk designation for mpox, particularly for Clade I transmission in Central Africa, where healthcare infrastructure limitations, population displacement, and inadequate vaccination coverage compound the biological risks of the disease itself.
For the general population in high-income countries, the risk of severe mpox disease remains low but is not negligible for specific groups. Individuals who are immunocompromised — including those living with HIV who are not on suppressive antiretroviral therapy — face a materially higher risk of severe disease and death. Sexual networks with high partner turnover represent a continued transmission pathway for Clade II, though the virus is not exclusively sexually transmitted and can spread through any prolonged close physical contact with infectious lesions or respiratory secretions.
The CDC’s testing pause, however temporary it may prove to be, risks creating surveillance gaps that could delay detection of new clusters or emerging variants — particularly in states with limited laboratory infrastructure.The epidemiological concern is not that mpox will suddenly accelerate in the absence of federal testing, but that delayed or missed diagnoses slow the public health response: contact tracing becomes harder, outbreak clusters go uncharacterized, and data quality feeding into national surveillance systems degrades. In the context of a pathogen with known potential for sustained human-to-human transmission, these are meaningful second-order risks.
Rabies — also included in the CDC’s testing pause — presents a different but equally serious concern given its near-universal fatality rate once symptomatic, underscoring that the pause’s impact extends well beyond mpox alone.
Prevention & Response
State public health laboratories are the immediate backstop for the CDC’s withdrawal from front-line mpox testing. According to CIDRAP’s reporting, these labs have stepped up to fill the gap, and many retain the technical capacity to conduct mpox polymerase chain reaction (PCR) testing established during the 2022 response. The practical challenge is one of volume, coordination, and ensuring that clinicians across the country are aware of where to send specimens and what the revised turnaround expectations are.
On the vaccine front, JYNNEOS (also marketed as Imvamune or Imvanex), the modified vaccinia Ankara-based vaccine licensed for mpox prevention, remains the primary immunization tool in the United States and across much of the developed world. The vaccine is administered as a two-dose series and has demonstrated strong efficacy against Clade II disease; its effectiveness against Clade I is biologically expected but has been studied under more limited conditions. Post-exposure prophylaxis protocols — administering the vaccine within days of known exposure — continue to be recommended for contacts of confirmed cases.
The WHO has maintained its global response framework, providing technical guidance to member states, supporting diagnostic capacity in resource-limited settings, and coordinating with the ECDC and regional partners on surveillance harmonization. In Central Africa, the response effort faces structural challenges that go beyond laboratory capacity: conflict-affected areas, displaced populations, and limited cold-chain infrastructure all complicate vaccination campaign delivery.
For clinicians in the United States, the practical guidance during the CDC testing pause is to contact state or local public health departments for specimen submission protocols. Physicians seeing patients with characteristic mpox presentations — vesicular or pustular rash, fever, lymphadenopathy — should not delay clinical suspicion pending federal guidance, and should engage with their state laboratory networks directly.
Public health messaging from the CDC has historically emphasized that mpox is preventable, that vaccines are effective, and that most cases in immunocompetent individuals are self-limiting over two to four weeks. Those messages remain accurate. What has changed, temporarily, is the institutional architecture supporting the detection and confirmation of new cases at the federal level — and the public health community’s ability to navigate that gap will depend heavily on the responsiveness and capacity of state laboratory systems that were not designed to operate as primary national reference infrastructure.
Sources
- European Centre for Disease Prevention and Control (ECDC) — Mpox Worldwide Overview (updated monthly): https://www.ecdc.europa.eu/en/mpox-worldwide-overview
- Center for Infectious Disease Research and Policy (CIDRAP) — “State public health labs step up as CDC pauses testing for various pathogens, including rabies, mpox” (April 3, 2026): https://www.cidrap.umn.edu/rabies/state-public-health-labs-step-cdc-pauses-testing-various-pathogens-including-rabies-mpox